Type of mutations
The recurrent de novo pathogenic mutation c.607C>T, p.(Arg203Trp) was found in heterozygosity, in the PACS1 gene, in almost all individuals described to date (Figure 2). There is one report of an individual with a de novo pathogenic substitution of the same amino acid: c.608G>A, p.Arg203Gln. It remains to be seen of other de novo mutation in PACS1 cause a similar, different or no phenotype at all.
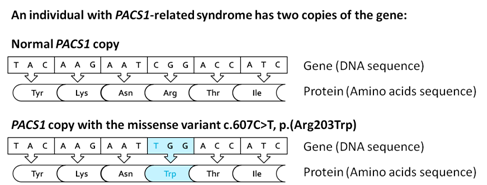
Figure 2. Pathogenic missense variant c.607C>T, p.(Arg203Trp) in one of the two copies of PACS1.
Genetic testing
The recurrent pathogenic variant c.607C>T is detected by sequencing analysis of the PACS1 gene.
Possible molecular diagnostic approaches to confirm the diagnosis in a proband include:
- performing a multi-gene panel, which includes PACS1, or performing exome sequencing, if multiple differential diagnosis exist.
- performing PACS1 Sanger sequencing (single-gene testing), if the clinical suspicion of PACS1-related syndrome is high.
Parents’ clinical evaluation and targeted genetic testing of identified variants (also the c.607C>T mutation) in the PACS1 gene is recommended to verify if the pathogenic variant identified in the proband was inherited or occurred de novo.
Suspected pathophysiologic mechanism
Previous animal studies suggested that the recurrent pathogenic variant c.607C>T results in an impaired function of the PACS1 protein.
Since PACS1 has a role in the migration of cranial neural crest, it was suggested that its impairment may lead to a defective migration of cells along the branchial arch, contributing to the craniofacial phenotype of individuals with PACS1-related syndrome.