Management and Surveillance
Currently, there is no known cure for a THOC2-related disorder. However, early intervention and education programs can maximise learning and social development, and medications can help manage some symptoms.
Close supervision by a paediatrician or physician experienced in caring for people with intellectual disability is recommended, so that appropriate educational and allied health support can be put in place.
Parents should be encouraged to promptly discuss any concerns about possible seizures, neurological symptoms (e.g. unsteady gait, tremor, movement disorder) or behavioural or mental health conditions with their child’s doctor so that these symptoms can be appropriately investigated and referral to a specialist (neurologist or psychiatrist) can be arranged.
- Suggested surveillance:
- Intellectual disability: Close developmental surveillance by a paediatrician/ physician with appropriate referral for early intervention and ongoing support at school and on school leaving.
- Increased risk of a seizure disorder: Review by paediatrician/GP/physician if any concerns regarding possible fits /’funny turns’/ blank episodes with a low threshold for referral to a neurologist/EEG.
- Possible increased chance of later onset neurological conditions: Assessment by a neurologist.
- Growth disorders: Height, weight and head circumference should be regularly measured and monitored in childhood, with consideration of referral to an endocrinologist if there is significant short stature. In adolescence/adulthood, weight and abdominal circumference should be regularly measured and monitored, with advice on weight management and referral to services such a dietitian if appropriate.
Genetic counselling
The majority of individuals with a THOC2-related disorder come from families that have a history of learning disabilities/ intellectual disability. These families are often referred to genetic services as the disorder has an X-linked pattern of inheritance.
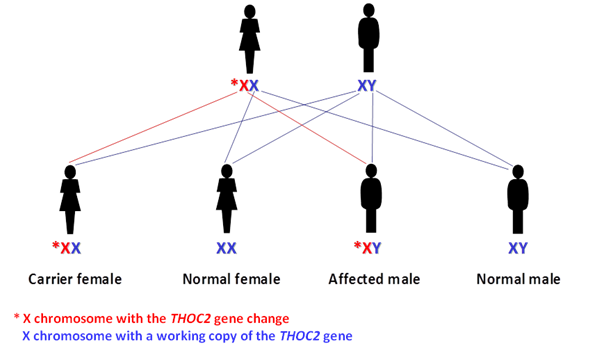
Males inherit an X chromosome from their mother and a Y chromosome from their father. Males who inherit an X chromosome with a THOC2 gene change will have a THOC2-related disorder. Females have two X chromosomes: one from their mother and one from their father and each X chromosome has a THOC2 gene. Females who have a gene change in one of their THOC2 genes are called carriers (see GOLD fact sheet ‘X-linked inheritance’).
A small number of individuals have been reported with a new [‘de novo’] change in the THOC2 gene, which is not present in the blood sample from their mother. These individuals typically come from families that have no family history of intellectual disability and the THOC2 gene change has occurred for the first time in the person with the disorder.
On occasion, one parent may have the THOC2 mutation (gene change) in some of their eggs or sperm cells but not be affected, as no other organ in their body has the mutation. This is called germline mosaicism and means that there is a very small chance that they may have another affected child. Referral to the genetics team to discuss this possibility can be helpful if planning another pregnancy.
What are the health implications associated with being a carrier of a THOC2 gene change?
Female carriers of a THOC2 gene change do not usually have intellectual disability or seizures, and are generally healthy. One female with a new (‘de novo’) genetic change in THOC2 has been reported, who was severely affected with intellectual disability and epilepsy. Information on more females with a change in the THOC2 gene is required in order to estimate the proportion of females who may be affected.
What are the chances of a female carrier having a child with a THOC2-related disorder?
When a female carrier is having children, for each pregnancy, there is a 50% chance of passing on the X chromosome with the working THOC2 gene and a 50% chance of passing on the X chromosome with the THOC2 gene change (see diagram).
Female carriers have choices when planning children and these options can be discussed with a clinical genetics service. Genetic counselling is available through a local genetic service when planning a pregnancy and in early pregnancy.
What are the chances of a male with a THOC2-related disorder having a child with the same disorder?
Males pass on their X chromosome to all their daughters and a Y chromosome to their sons. While it is unlikely that a male with a THOC2-related disorder with moderate or severe intellectual disability will partner and have children, those that are more mildly affected could have children and would pass on the X chromosome with the THOC2 gene change to all of their daughters. This means all their daughters will be carriers and have a chance of having sons of their own with a THOC2-related disorder. As a male with a THOC2 disorder passes on his Y chromosome to all his sons they will not be carriers or have a THOC2-related disorder.