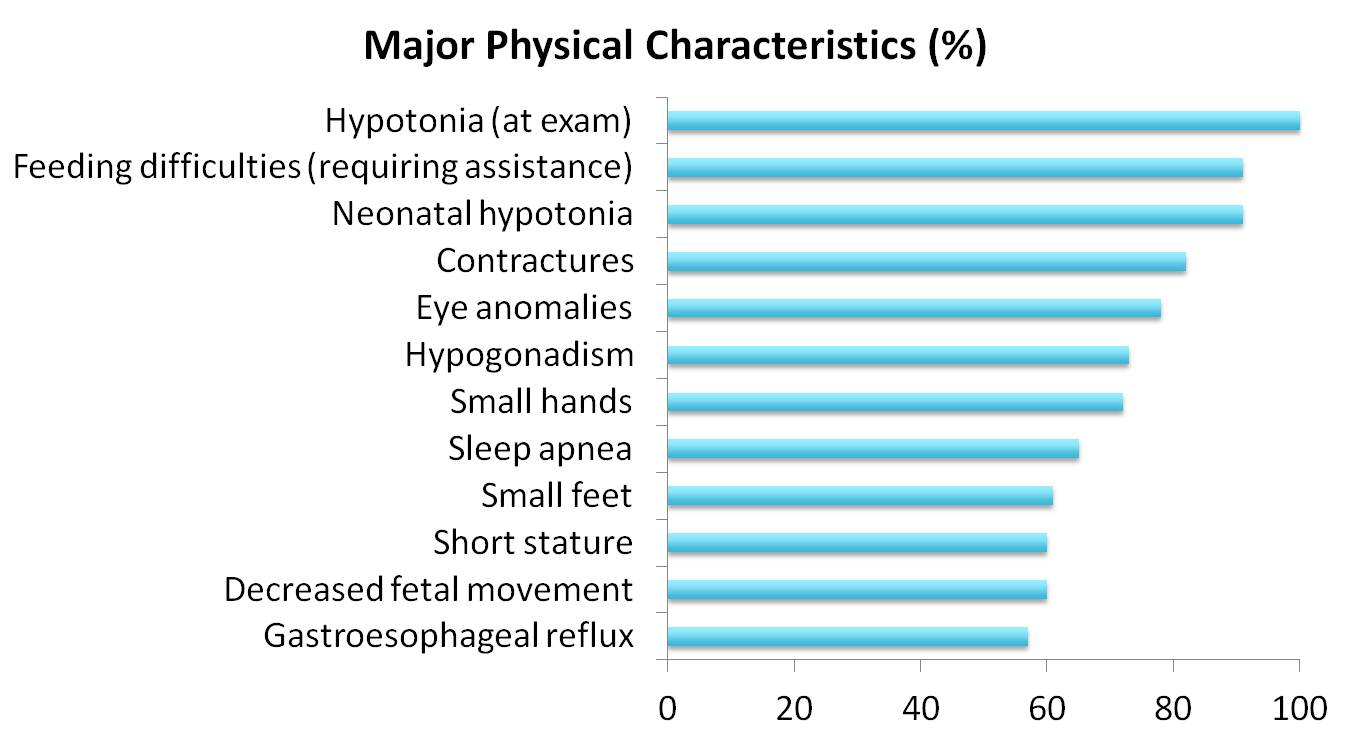
Primary clinical features include hypotonia, feeding difficulties requiring assisted feeding techniques, and contractures of the interphalangeal joints, which can present very early in life and can be important in establishing a diagnosis. Further phenotypes seen with prevalence greater than 50% include eye anomalies (strabismus, myopia, esotropia), hypogonadism, small hands, small feet, short stature, sleep apnea, decreased fetal movement, and gastroesophageal reflux. While facial dysmorphisms of frontal bossing, short philtrum, bushy eyebrows, and prognathia, are commonly noticed, there is great variability in these dysmorphic features.
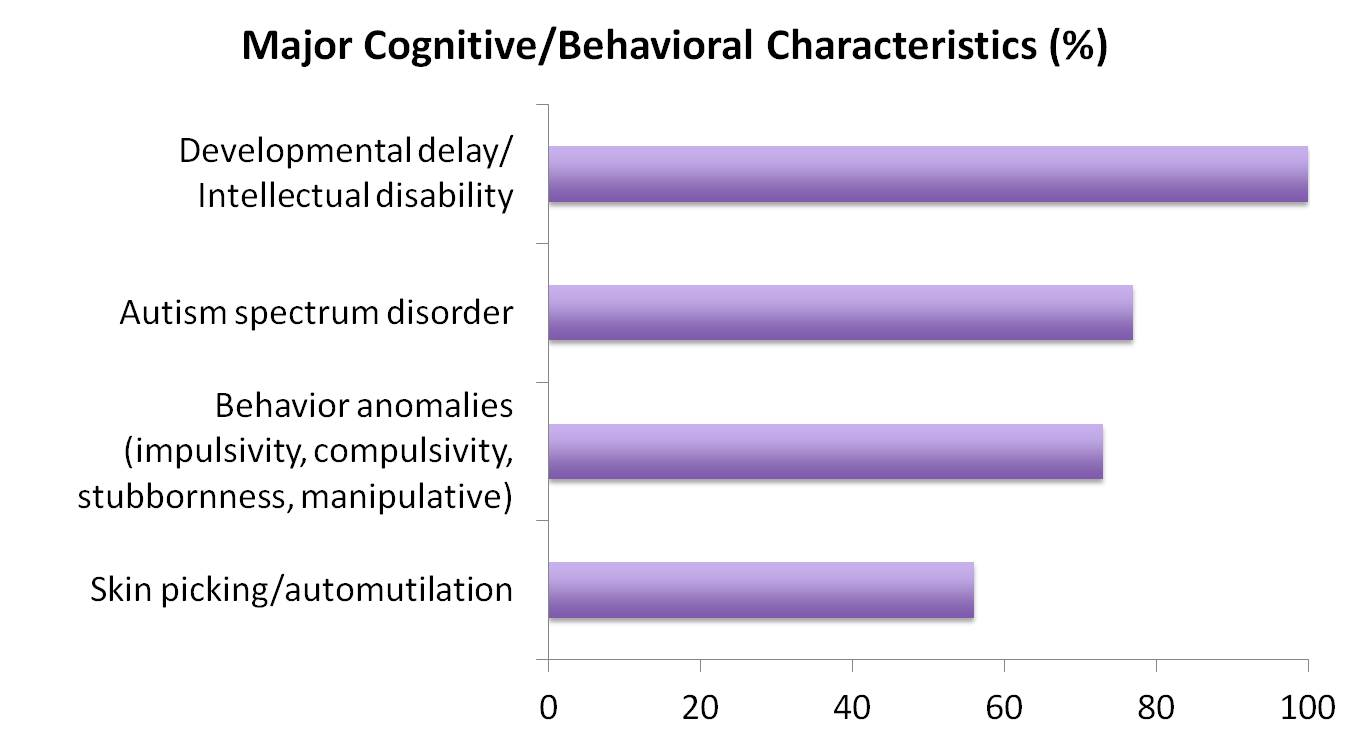
Cognitive and behavioral characteristics are frequently seen in association with Schaaf-Yang syndrome. These include developmental delay and intellectual disability, autism spectrum disorder and/or signs of autism, behavioral anomalies in the form of impulsivity, compulsivity, stubbornness, and manipulative behaviors. Skin picking/automutilation is frequently seen.
Differential diagnosis
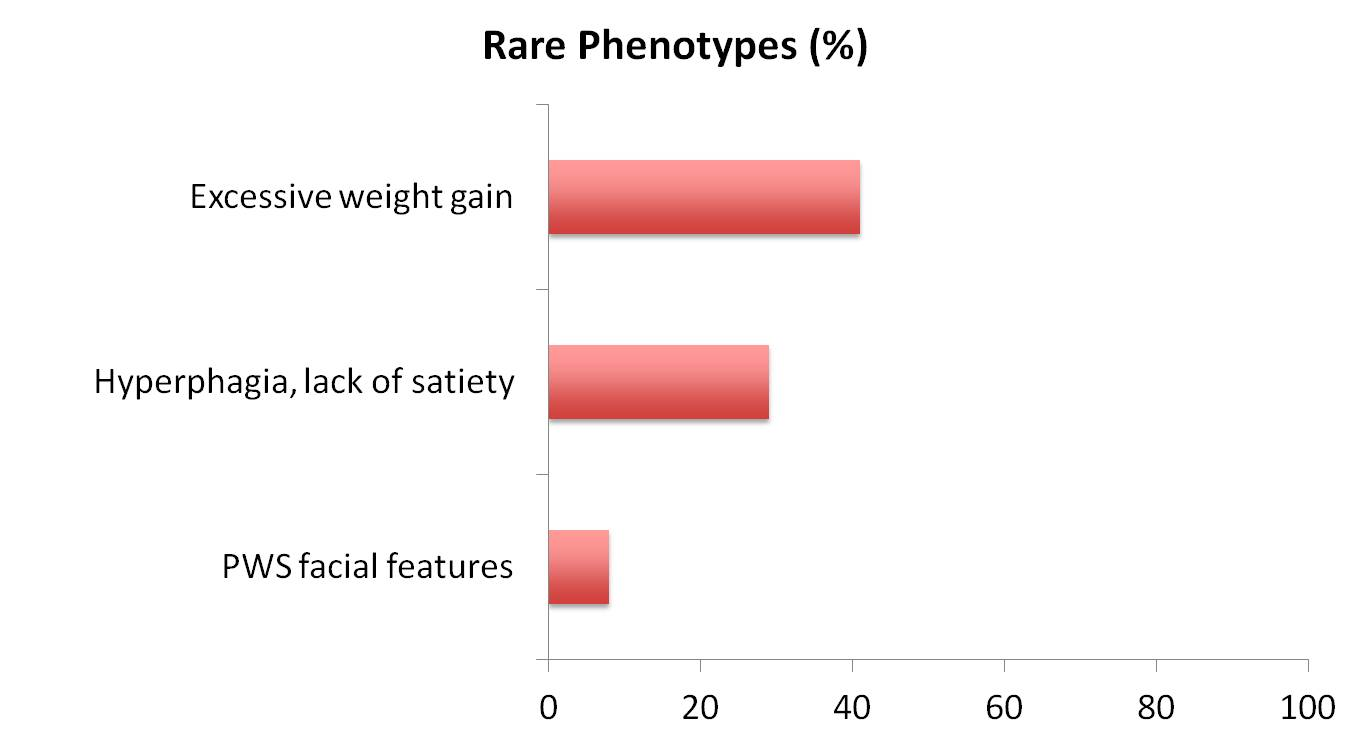
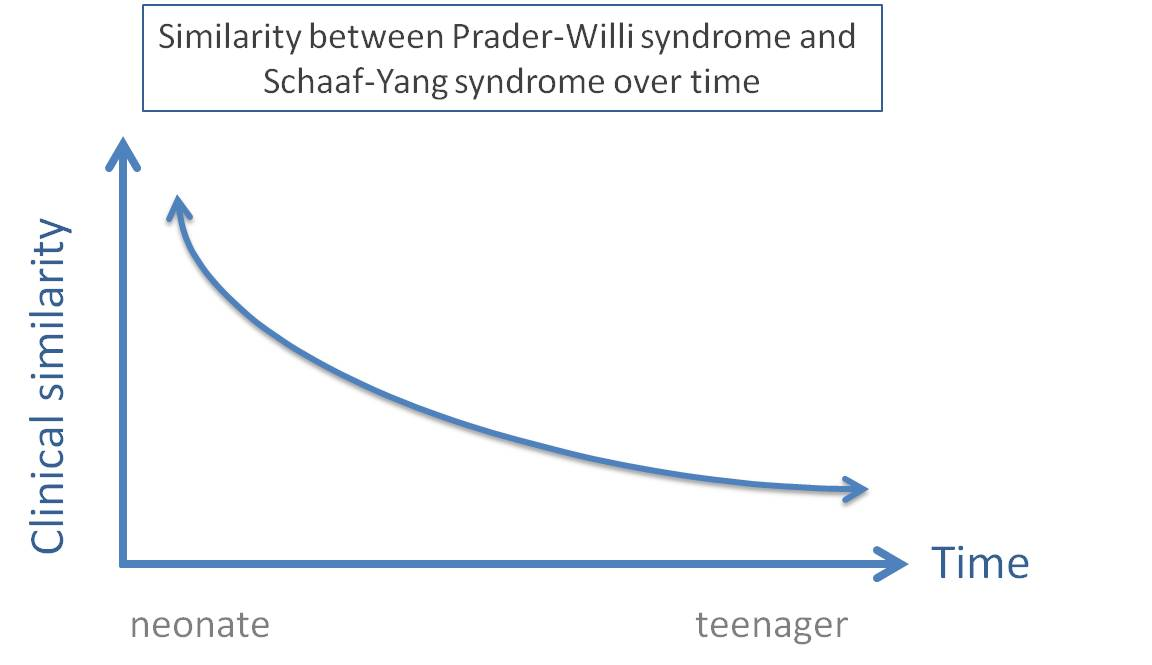
When considering Schaaf-Yang syndrome as a differential diagnosis for Prader-Willi syndrome, it is critical to note that excessive weight gain, hyperphagia, and Prader-Willi syndrome characteristic facial features are seen only in a minority of cases of Schaaf-Yang syndrome.
Genotype-Pheotype correlation
Schaaf-Yang syndrome exhibits a variable expressivity of phenotypes. Some of the most severe phenotypes have been reported in conjunction with the specific mutation c.1996delC (p.Q666fs) in the MAGEL2 gene. Affected individuals manifested fetal akinesia and severe arthrogryposis, along with multiple pterygia, talipes equinovarus, and retro-micrognathia.